


1Lübeck Institute of Experimental Dermatology, University of Lübeck, Lübeck, 2Department of Dermatology, Case Western Reserve University, Cleveland, OH, USA, 3Clinical Dermatology, IRCCS Istituto Ortopedico Galeazzi, 4Department of Biomedical, Surgical and Dental Sciences, University of Milan, Milan, Italy, and 5Clalit Healthcare Services, Tel-Aviv, Israel
Although pemphigus has recently been linked to psoriasis, the risk of emergence of pemphigus during the course of psoriasis is yet to be delineated. The aim of this study was to evaluate the risk of developing pemphigus during the course of psoriasis. A large-scale population-based longitudinal retrospective cohort study was performed to assess the hazard ratio (HR) of pemphigus among 68,836 patients with psoriasis relative to 68,836 age-, sex-, and ethnicity-matched controls. The incidence of pemphigus was 0.14 (95% confidence interval (95% CI) 0.10–0.19) and 0.04 (95% CI 0.02–0.07) per 1,000 person-years among psoriatic patients and controls, respectively. Patients with psoriasis were more than 3 times as likely to develop pemphigus (HR 3.25; 95% CI 1.70–6.21). The increased risk remained statistically significant following adjustment for several confounders (adjusted HR 3.19; 95% CI 1.67–6.11). To conclude, psoriasis is associated with an elevated risk of pemphigus. Further research is needed to explore the immunoserological profile of patients with a dual diagnosis.
Key words: psoriasis; pemphigus; cohort study.
Accepted Jul 9, 2020; Epub ahead of print Jul 31, 2020
Acta Derm Venereol 2020; 100: adv00293.
doi: 10.2340/00015555-3607
Corr: Khalaf Kridin, Lübeck Institute of Experimental Dermatology, University of Lübeck, Building #32, Ratzeburger Allee 160, DE-23562 Lübeck, Germany. E-mail: dr_kridin@hotmail.com
This large-scale cohort study included 68,836 patients with psoriasis and 68,836 matched controls. Patients with psoriasis were found to have a three-fold increased risk of developing pemphigus during the course of their disease. Physicians managing patients with psoriasis should be aware of this association and monitor psoriatic patients for the occurrence of pemphigus. Further research is required to delineate the mechanism underlying this association.
Psoriasis is a chronic papulosquamous dermatosis caused by dysregulation of the immune system, manifesting morphologically with scaly erythematous plaques. This disease is typified by substantial physical and psychological burdens for patients (1, 2). While it is widely accepted that inflammation driven by tumour necrosis factor-α/interleukin-23/interleukin-17 axis is the key mechanism underlying the development of psoriasis, it also possesses an autoimmune facet that manifests as autoreactive T cells (3). The association of psoriasis with bullous pemphigoid, vitiligo, and thyroiditis lends credibility to this notion (3).
Pemphigus encompasses a group of rare, potentially devastating, intraepidermal autoimmune blistering dermatoses (4). It manifests clinically with vesicles and erosions on the skin and mucosae, often impairing the patient’s quality of life and causing increased morbidity and lethality (5, 6). The pathogenesis arises from the production of immunoglobulin G (IgG) autoantibodies against desmoglein 3 and desmoglein 1, epidermal cadherin-type cell-cell adhesion molecules (7). Several studies have verified the validity of the “autoimmune diathesis” concept in pemphigus, by demonstrating its association with an array of autoimmune diseases (4).
While psoriasis is associated with bullous pemphigoid, a relatively common subepidermal autoimmune organ-specific blistering disease (8–10), its association with pemphigus was only recently suggested by a handful of epidemiological studies. Three cross-sectional studies evaluated the prevalence of psoriasis among patients with pemphigus relative to control individuals (6, 11, 12,). Data from these studies were subsequently synthesized in a meta-analysis, revealing a pooled odds ratio (OR) of 3.5 (95% confidence interval (95% CI) 1.6–7.6) for psoriasis in patients with pemphigus (13). The inverse association was evaluated only in a single study tracking psoriatic patients (14). To date, knowledge about the risk of developing incident pemphigus during the course of psoriasis is yet to be established.
The aim of the current study was to further investigate the association between psoriasis and pemphigus, by conducting a large-scale retrospective cohort study evaluating the risk of developing pemphigus among patients with underlying psoriasis.
Study design and database
A retrospective cohort study was conducted aiming to identify the risk of the occurrence of incident pemphigus among patients with psoriasis relative to control individuals.
This study was based on the electronic dataset of Clalit Healthcare Services (CHS). CHS is the largest Israeli healthcare provider, providing both public and private healthcare services to approximately 4,400,000 enrollees as of 2016 (constituting approximately 54% of Israel’s general population, consistent with the 2016 census). The computerized dataset of CHS is typified by constant real-time input from medical, administrative, and pharmaceutical operating systems and was proven effective to facilitate the performance of epidemiological studies.
The chronic disease registry of CHS collects data from multiple sources, including from primary care and hospital reports, and is then manually confirmed by primary care physicians. This registry is regarded as reliable (15).
Study population and covariates
Both psoriasis and pemphigus diagnoses were defined by the following criteria: a documented diagnosis of these conditions at least twice in the medical records, as documented by community physicians, or when hospital discharge documentation registered these diagnoses. The control group consisted of one patient matched to the corresponding case by age, sex, and ethnicity. Age was matched based on the exact year of birth (1-year strata).
Outcome measures were adjusted for comorbid diseases by use of the Charlson comorbidity index, a validated method of measuring comorbid underlying diseases, which has been demonstrated as a dependable predictor of mortality (16). Socioeconomic status (SES) was defined according to the poverty index of the member’s residence area, as defined during the 2008 National Census in Israel (https://www.cbs.gov.il/he/Statistics/Pages/?--?-2008.aspx). The population was divided into 3 categories according to their poverty index (low, intermediate, and high).
Statistical analysis
Baseline characteristics are described by means and standard deviations (SD) for continuous variables, whereas percentages are used to describe categorical values. The distribution of clinical and sociodemographic factors was compared between psoriatic patients and controls using χ2 test and t-test, as indicated.
The incidence rates of pemphigus were calculated for both psoriasis patients and controls and expressed as the number of events per 1,000 person-years. Hazard ratios (HRs) for the risk of incident pemphigus were calculated by the use of Cox regression models. The incidence of pemphigus during follow-up was obtained only for individuals without a history of pemphigus prior to study initiation. Results with 95% CI were reported where applicable. Two-tailed p-values < 0.05 were regarded as of statistical significance. SPSS software, version 25 (SPSS, Armonk, NY, USA: IBM Corp.) was utilized to conduct all statistical analyses.
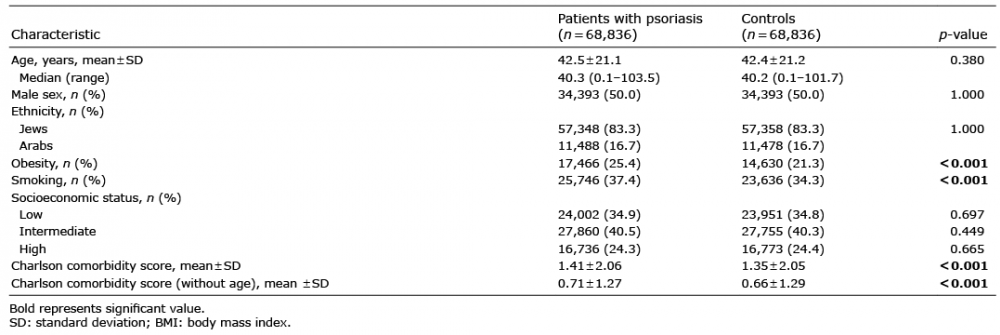
The study population comprised 68,836 consecutive incident patients with psoriasis, and 68,836 control individuals who were matched according to age, sex, and ethnicity (Table I). The mean ± standard deviation (SD) age at the onset of psoriasis and recruitment of controls was 42.5 ± 21.1 and 42.4 ± 21.2 years, respectively, and 50.0% of the study populations were females. No significant variability in the socioeconomic status was observed between the 2 groups. Compared with control individuals, patients with psoriasis had a higher prevalence of obesity (25.4% vs. 21.3%; p < 0.001) and smoking (37.4% vs. 34.3%; p < 0.001). The mean ± SD Charlson comorbidity score was higher in patients with psoriasis relative to control participants (1.41 ± 2.06 vs. 1.32 ± 2.05, respectively; p < 0.001). The characteristics of the case and control groups are detailed in Table I.
Table I. Descriptive characteristics of the study population
During the follow-up period, a total of 39 and 12 patients developed new-onset pemphigus, among the case and control groups, respectively. The mean ± SD latency from the diagnosis of psoriasis until the emergence of pemphigus was 2.0 ± 1.8 years. The total follow-up time was 273,275.0 person-years for patients with psoriasis and 273,333.6 person-years for controls. Altogether, the incidence rate of pemphigus was 0.14 (95% CI 0.10–0.19) and 0.04 (95% CI 0.02–0.07) per 1,000 person-years among patients with psoriasis and controls, respectively.
The crude risk of pemphigus was more than threefold higher in patients with psoriasis than in control individuals (HR 3.25; 95% CI 1.70–6.21). In subgroup analysis, the crude risk of pemphigus was elevated both among female (HR 4.20; 95% CI 1.58–11.14) and male (HR 2.57; 95% CI 1.07–6.16) patients. After controlling for confounders, including sex, age, socioeconomic status, ethnicity, and comorbidities, psoriasis remained an independent significant risk factor for incident pemphigus (adjusted HR 3.19; 95% CI 1.67–6.11; Table II).
A dual diagnosis of psoriasis and pemphigus does not significantly increase the risk of all-cause mortality compared with that observed among patients with isolated psoriasis (HR 1.37; 95% CI 0.78–2.43).
Table II. Hazard ratios (HRs) of new-onset pemphigus among patients with psoriasis and control subjects
The current large-scale population-based retrospective cohort study demonstrated that patients with psoriasis are more than 3 times as likely to develop new-onset pemphigus as control individuals (HR 3.25). The risk is particularly higher among female patients with psoriasis (HR 4.20).
Current knowledge about the association between psoriasis and pemphigus
Three cross-sectional studies tracked patients with pemphigus to examine the association between pemphigus and psoriasis. In their large-scale study of 1,985 patients with pemphigus and 9,874 controls, Kridin et al. (11) reported that Israeli patients with pemphigus are associated with a 2.6-elevated odds of psoriasis (multivariate OR, 2.6; 95% CI 1.9–3.6). Analysing large health insurance data of 6,406 patients with pemphigus from the USA, Hsu et al. (6) found a multivariate OR of 2.2 (95% CI 1.5–3.2) to be diagnosed with psoriasis. Chiu et al. (12) analysed the data of 1,998 patients with pemphigus and 7,992 controls from Taiwan and observed an even higher multivariate OR of 7.2 (95% CI 5.6–9.3). In the current meta-analysis synthesizing data from the 3 aforementioned studies, we concluded that the combined odds for psoriasis was 3.5-fold increased (pooled OR 3.5; 95% CI 1.6–7.6) among patients with pemphigus (13). A principal drawback stems from the cross-sectional nature of these studies, which hampers the identification of the temporal relationship between the 2 studied conditions. This obviously interferes with drawing firm conclusions regarding a causal relationship between these entities (17), and complicates the understanding of the pathomechanism underlying the observed association.
As for the cohort of patients with psoriasis, evaluation of the association with pemphigus was performed in only one cross-sectional Taiwanese study. This study consisted of 51,800 psoriatic patients and noted that the prevalence of pemphigus was higher in cases than in healthy control individuals (OR 41.8; 95% CI 12.4–140.9) (14). However, given that the association is yet to be investigated in studies conducting a longitudinal follow-up, the risk of emergence of incident pemphigus in patients with psoriasis is unknown. In a Japanese study aiming to characterize 145 patients with coexistent autoimmune blistering diseases and psoriasis, pemphigus foliaceus was reported in 2.8% of the eligible patients (18).
Biologic mechanism of the observed association
The pathomechanism underlying the increased occurrence of pemphigus among patients with psoriasis is not yet fully elucidated. However, several hypotheses had been postulated to account for this association. The pathogenesis may be attributed to the “epitope-spreading phenomenon”, where the primary inflammatory process of psoriasis may induce changes in epidermal proteins, thus exposing certain epitopes that were formerly hidden from the immune system. This process may finally induce a secondary autoimmune humoral response (19). It has also been argued that alteration in the regulation of T cells leading to increased generation of autoantibodies might be a reasonable link interpreting the coexistence of both conditions in particular individuals (20).
Plasminogen activator levels have been proven to be elevated in psoriatic lesions. Intriguingly, activation of plasminogen is recognized to take part in the acantholytic process in pemphigus (20–22). Some authors have assumed that inflammation from other dermatoses might form a suitable environment for the expression of intraepidermal antigens and enhance the activity of pathogenic autoantibodies of pemphigus (20, 23). The role of genetic predisposition may also be weighted, given that the HLA DRB1 allele has been reported to associate with both pemphigus (24) and psoriasis (25). Additional genetic studies may contribute to further clarify the pathomechanism underlying this clinical observation.
The occurrence of pemphigus may also stem from anti-psoriatic therapies, particularly ultraviolet (UV) irradiation. Several anecdotal reports have suggested that heat and sunlight may confer an aggravating role in pemphigus (26–30). Correspondingly, UV irradiation was found to cause epidermal instability and even acantholysis in non-lesional skin of patients with pemphigus, which may lend weight to the triggering role of UV in psoriatic patients managed by phototherapy (30). Unfortunately, the current study was not able to adjust for this variable in the analysis.
Strengths and limitations
The current study answers a novel epidemiological question regarding the longitudinal risk of developing pemphigus among patients diagnosed with psoriasis. The inclusion of a large-study population enables identification of the association with an uncommon disease such as pemphigus, which is not methodologically feasible in smaller studies. The large sample size and the presence of patients originating from both community and hospital settings diminish the risk of selection bias. However, the current study has some limitations. The diagnosis of pemphigus was not immunopathologically validated, and the clinical characteristics of eligible cases and the subtypes of psoriasis could not be retrieved. In addition, we are not able to adjust the outcome measure of interest to anti-psoriatic therapies, namely phototherapy, which may pose a confounding factor. Although statistically significant, the crude risk of pemphigus among psoriatic patients is still relatively low.
Conclusion
The current retrospective cohort study provided evidence that Israeli patients with psoriasis are at more than threefold increased risk of developing pemphigus during the course of their disease. Physicians managing patients with psoriasis should be aware of this epidemiological feature. Prospective studies are required to establish this association in other ethnic populations. Experimental studies will be of help to better comprehend the mechanisms underlying this observation.


 Click to show fullsize
Click to show fullsize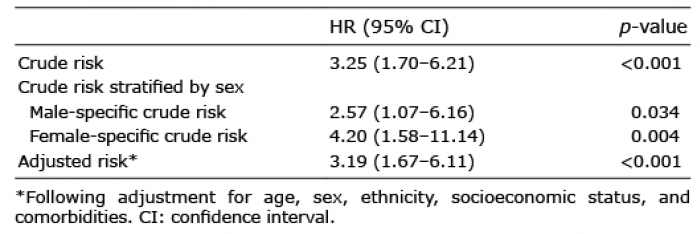 Click to show fullsize
Click to show fullsize